
{kind=link}
Newsweek names 11 UF Health specialists top in cancer care
Cancer is a complex and varied disease. It can begin anywhere in the body and spread for reasons that are not yet understood. Even the same kind of cancer can…

Update your location to show providers, locations, and services closest to you.
For patients with clinically localized prostate cancer, nerve-sparing robotic prostatectomy provides patients with a safe and minimally invasive technique for removal of the prostate gland, while preserving as much of the surrounding nerve structures responsible for penile erections.
This minimally invasive approach has the advantage of smaller incisions, reduced pain, blood loss, transfusion rates and hospital stay, as compared to conventional open surgery with a similar cure rate. In select patients with locally invasive or metastatic cancer, morbid obesity, bleeding tendencies, or severe heart or lung problems, robotic prostatectomy may not be advised.
Robotic prostatectomy requires that patient undergo a general anesthesia. While operative time varies from one individual to another, the average operating time is approximately 3-4 hours.
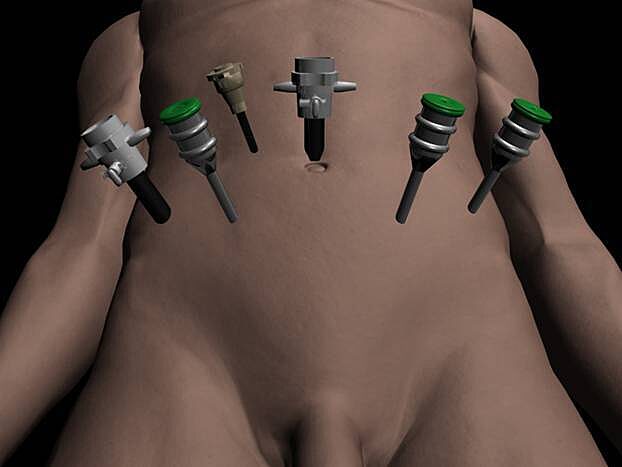
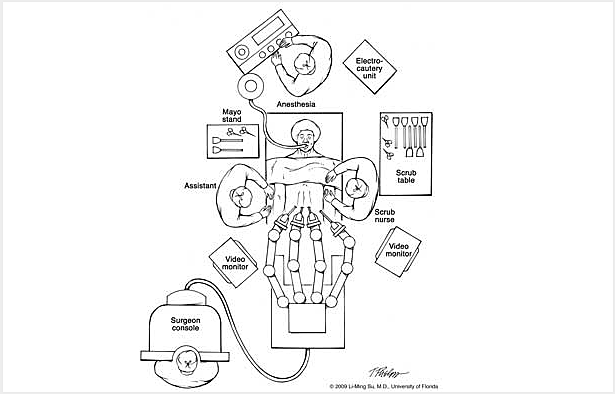
During robotic prostatectomy approximately 6 small keyhole (< 1cm) incisions are made in the abdomen (Figure 1), through which portals or trocars are placed to allow passage of instrumentation into the abdomen.
The abdomen is filled with carbon dioxide gas to create a larger working space for the surgeon to accomplish the operation. This gas is later evacuated from the abdomen at the conclusion of the operation. The surgeon controls 3 multi-jointed robotic instruments to accomplish the tasks of dissection, cauterization, cutting and suturing with the same dexterity as the human wrist (Figure 2).
In addition, the surgeon controls a stereoscopic lens connected to a high definition camera which provides a three dimensional, high definition view of the internal anatomy. A highly skilled surgical assistant stands at the operating table assisting the surgeon by exposing and retracting tissue using instrumentation inserted through two of the trocars.
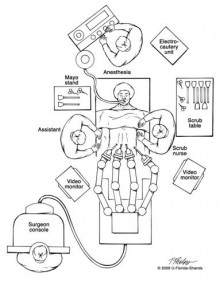
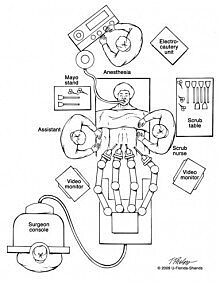
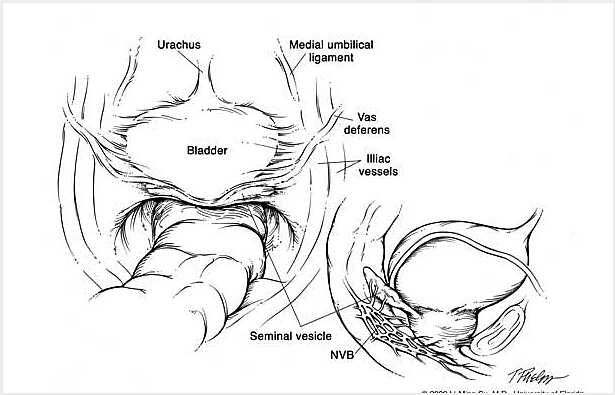
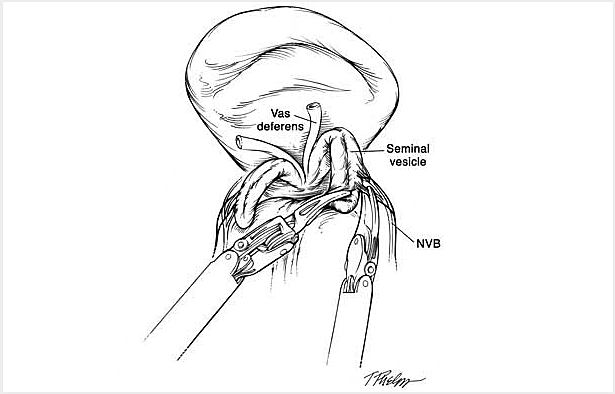
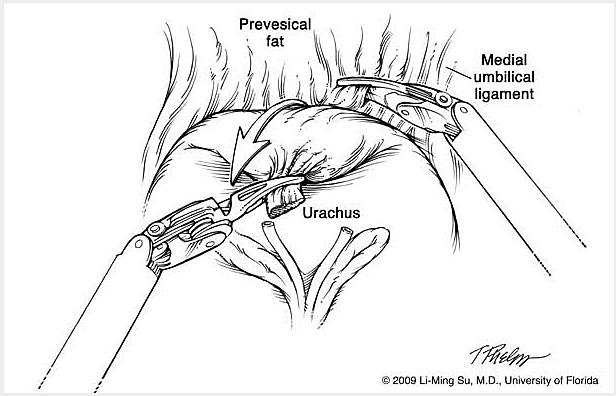
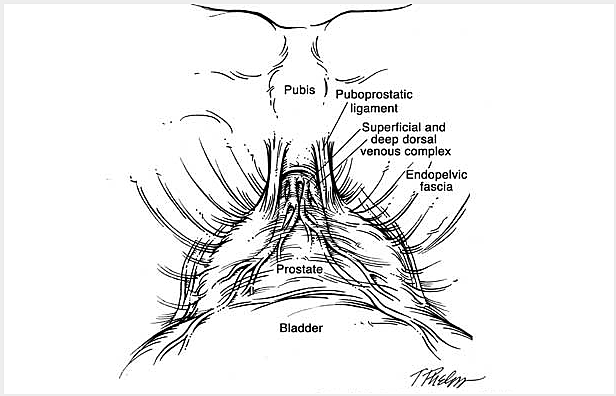
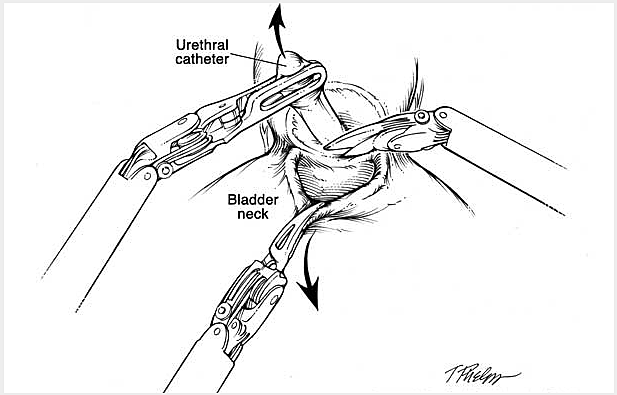
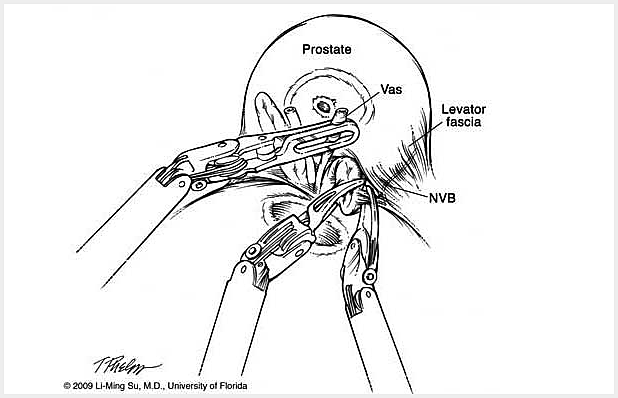
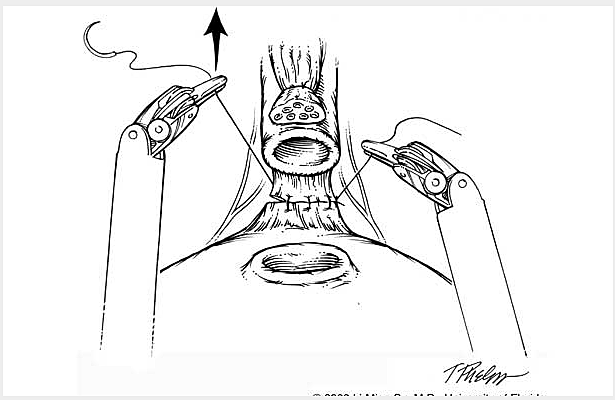
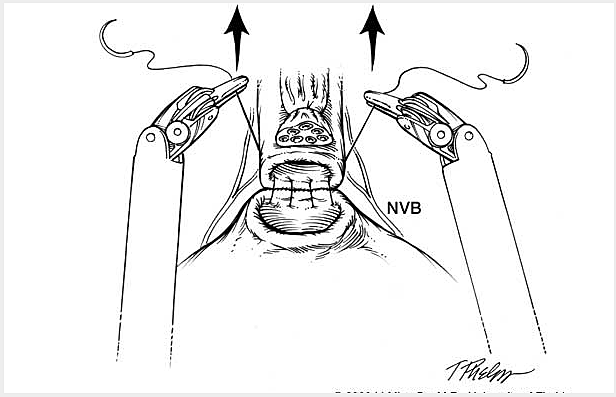
The da Vinci S Surgical Robotic System is assembled to the trocars prior to commencing the operation. With the operating surgeon seated a few feet away at the surgeon operating console, the robotic instrumentation is controlled by the surgeon in real time with highly precise motion scaling (Figure 3-1 & FIgure 3-2).The prostate gland, seminal vesicles and vas deferens are then dissected and exposed (Figure 4).


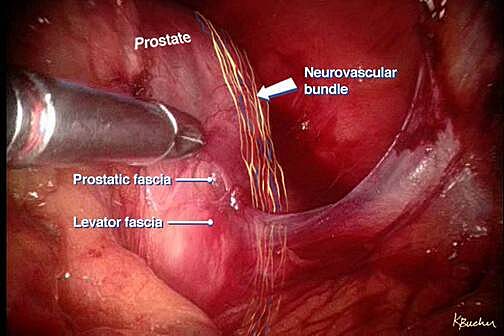
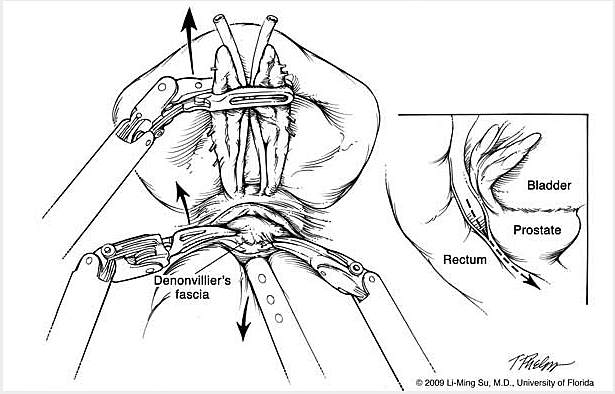
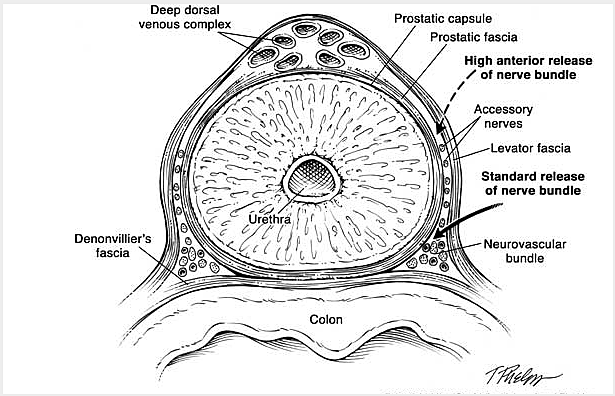
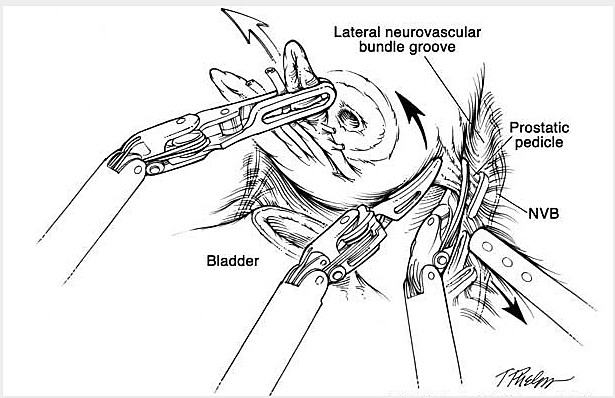
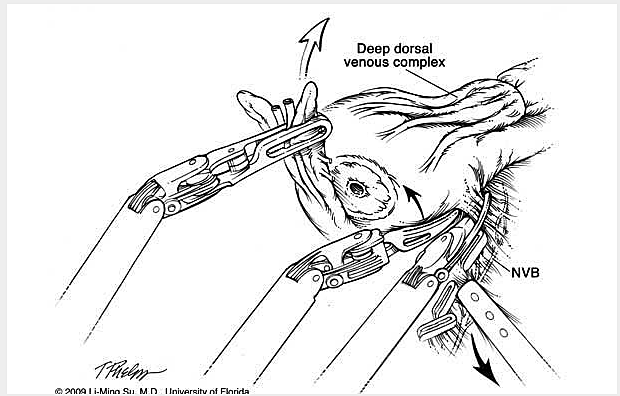
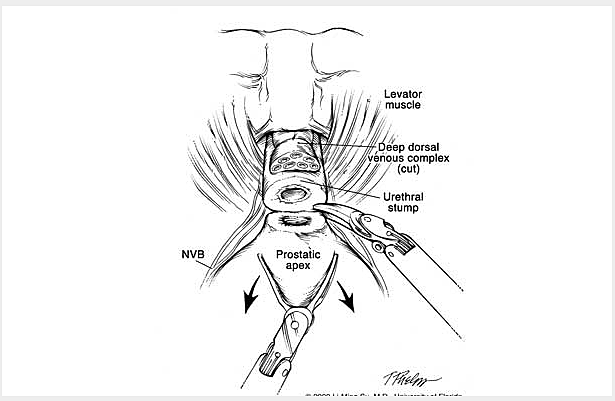
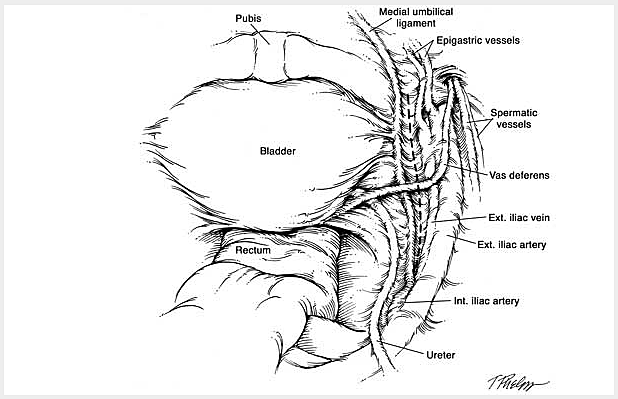
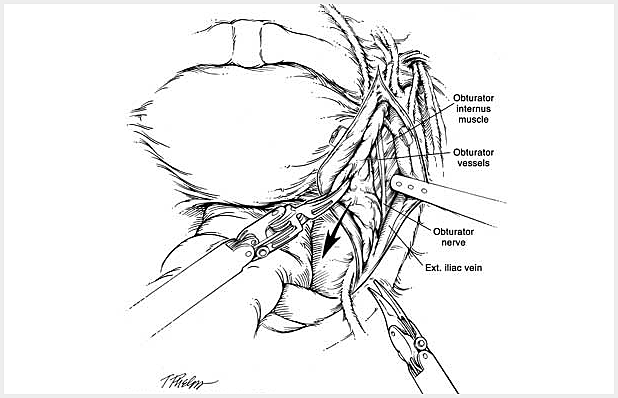
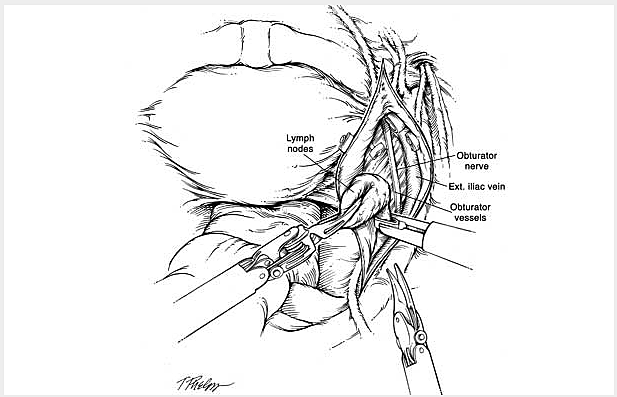
Pelvic lymph nodes that may be involved by cancer are removed when indicated to better stage the extent of tumor involvement. Lastly the bladder is sewn back to the urethra to restore continuity of the urinary tract. Thermal energy is minimized during dissection of the prostate so as to avoid injury to the delicate nerve fibers and muscles involved in penile erections and urinary control. Once the prostate and lymph nodes are removed, they are immediately placed within a plastic sack which is later removed intact at the end of the operation through an extension of one of the existing abdominal incision sites. A small drain is left at the end of the procedure exiting one of the keyhole incisions along with a urethral catheter (called foley), which is used to bridge the connection created between the bladder and urethra (called the anastomosis). Finally the specimens are removed from the abdomen through the plastic entrapment sack and the skin incisions closed using plastic surgery techniques to minimize scarring. Abdominal incisions at one month following surgery are generally barely visible.
The following is a slide show of a series of schematic drawings to help patients better understand the steps involved with nerve-sparing robotic prostatectomy.
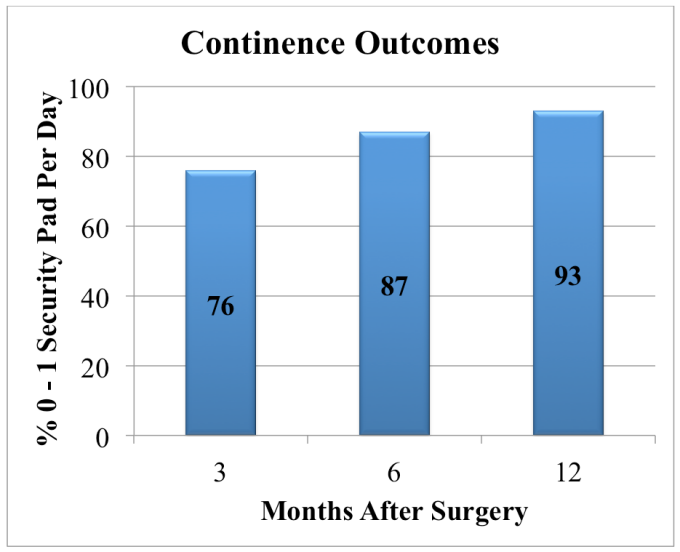
Although most patients experience some degree of urinary leakage (i.e. incontinence) following robotic prostatectomy, most patients quickly regain control by 3-6 months following surgery. (Figure revised from: Willis DL, Gonzalgo ML, Brotzman M, Feng Z, Trock B and Su LM. Comparison of outcomes between pure laparoscopic vs robot-assisted laparoscopic radical prostatectomy: a study of comparative effectiveness based upon validated quality of life outcomes. Br J Urol Int 109: 898-905, 2012).
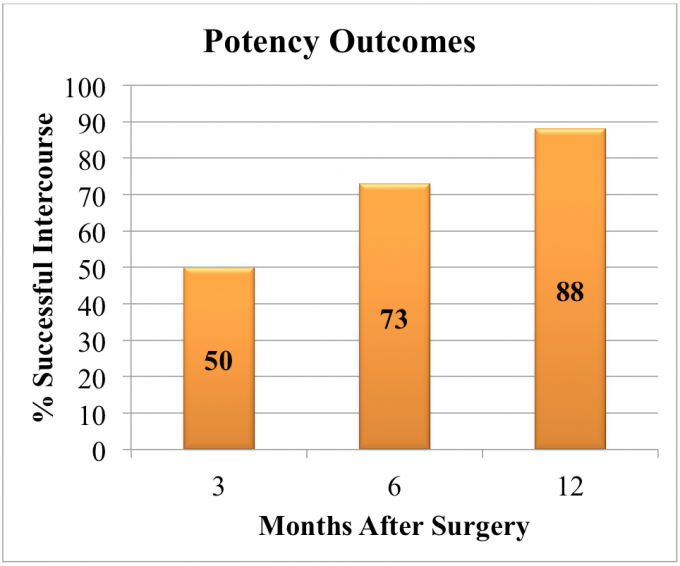
Return of sexual function following nerve-sparing robotic prostatectomy is more challenging to define and assess as results depend on multiple factors including patient age, preoperative sexual function, percent of nerves spared during surgery, recovery time after surgery and presence of pre-existing medical conditions such as hypertension, heart disease, diabetes, obesity, smoking and high cholesterol. Based upon validated quality of life surveys and of patients who were fully potent preoperatively who underwent bilateral nerve preservation, 50%, 73% and 88% of patients reported successful intercourse with or without the use of phosphodiesterase 5 inhibitors (i.e. Viagra, Cialis, Levitra) at 3, 6, and 12 months postoperatively. (Figure revised from: Willis DL, Gonzalgo ML, Brotzman M, Feng Z, Trock B and Su LM. Comparison of outcomes between purle laparoscopic vs robot-assisted laparoscopic radical prostatectomy: a study of comparative effectiveness based upon validated quality of life outcomes. Br J Urol Int 109: 898-905, 2012).
As with any major surgery, complications, although rare, may occur with robotic prostatectomy. Potential risks and complications with this operation include but are not limited to the following:
After a period of recovery in the Recovery Room, you will be transported to your hospital room once you are aware and your vital signs stable.
Robotic laparoscopic prostatectomy is used to treat patients who have clinically localized prostate cancer. Most patients who are candidates for open radical prostatectomy are also excellent candidates for the robotic approach. In many centers including the University of Florida, the robotic approached is the treatment of choice for the surgical management of clinically localized prostate cancer.
Patients with a history of extensive abdominal surgery, radiation, pre-existing heart or lung disease, morbid obesity, or bleeding tendencies may not be the best candidates for robotic prostatectomy. Patients with know metastatic or recurrent prostate cancer are not candidates for robotic prostatectomy. Although patients with very large prostate glands (e.g. > 100 grams) can undergo robotic prostatectomy, operative times are generally longer than in patients with smaller prostate gland sizes.
The primary advantages of robotic prostatectomy are a result of the high tech equipment used to accomplish this surgery. First, there is improved visualization with 10-12 X magnification and a high definition view of the internal anatomy as a result of the use of a specialized stereoscopic endoscope lens which is connected to a high definition camera.
Second, robotic surgeons operate with multi-jointed 8 mm instruments which have the same dexterity as the human wrist. Taken together robotic surgery provides better visualization of the critical structures surrounding the prostate gland and allows surgeons to operate with the same flexibility and ease as an open surgeon has when performing open prostatectomy, while at the same time accomplishing this through smaller incisions with significantly reduced blood loss.
Our robotic surgeons have all received extensive advanced fellowship training in laparoscopic and robotic surgery and have been performing robotic prostatectomy since 2002.
Robotic prostatectomy generally takes 2-4 hours depending on many factors including size of the prostate gland, presence of obesity, prior abdominal surgery and scar tissue, and other factors. Many of these pre-existing factors mandate a longer operative time. Our surgeons focus on performing a thorough and meticulous surgery and not on speed of the operation.
Although extremely rare, conversion to open surgery may be required if difficulty with dissection or extensive bleeding is encountered during the robotic approach.
Our surgeons are trained in open surgical approaches as well as laparoscopy and robotic surgery and therefore are well equipped to complete the surgery in an laparoscopic or open fashion if needed.
Success rate in complete removal of cancer is similar to the open surgical approach. Prognosis of cancer-free survival is multifactorial and is based in part upon the grade and stage of your cancer and will be discussed with you by your surgeon following surgery during review of the pathology report. In our experience, only 4.8% of patients with organ confined disease (i.e. stage pT2) had positive surgical margins and 23.7% of patients with locally advanced disease (i.e. ≥ stage pT3).
The timing and extent of return of urinary continence and sexual potency following prostatectomy is a complex process that is time dependent and multifactorial. Some of the factors that influence the success of return of these quality of life issues include patient factors such as age, preoperative urinary and sexual function, and presence of medical conditions such as hypertension and diabetes. In addition, surgical factors such as quality and quantity of nerve preservation can influence outcomes.
For young patients (<60 years old) who were preoperatively potent with no urinary issues who receive bilateral nerve preservation, 80% and 93% were continent (defined as 0-1 security pad) and 72% and 85% were potent (defined as having the ability to engage in intercourse with or without the use of phosphodiesterase inhibitor medications) at 6 and 12 months respectively. These results can vary significantly dependent on individual circumstances including extent of cancer, age, and comorbid medical conditions.
For patients with organ confined prostate cancer that has not spread beyond the prostate capsule or into the lymph nodes or seminal vesicles, prognosis remains excellent as most are cured with surgery alone. In cases where more invasive or metastatic disease is found, additional treatments including radiation and hormonal therapy may be required. There are clinical trials with chemotherapy and vaccine therapy that are available at our institution for cases of metastatic prostate cancer that are refractory to conventional treatments. These would be administrated under advisement of a medical oncologist.
University of Florida robotic surgeons are involved in several exciting research projects pertaining to robotic pertaining to robotic prostatectomy. First, we are involved with prospective collection of perioperative outcomes for each patient undergoing robotic prostatectomy. In this way, our robotic surgeons track quality of life and cancer outcomes following surgery to assess trends in outcomes and the effects of changes in surgical technique or new technology on these outcome measures. Second, we are investigating new imaging modalities to identify the precise course and location of the neurovascular bundles as well as cancer sites during this procedure using novel MRI technology. Lastly we are developing a robotic surgical simulator to help better prepare and train residents and fellows on the technical nuances of robotic surgery.

Cancer is a complex and varied disease. It can begin anywhere in the body and spread for reasons that are not yet understood. Even the same kind of cancer can…